Click below to register
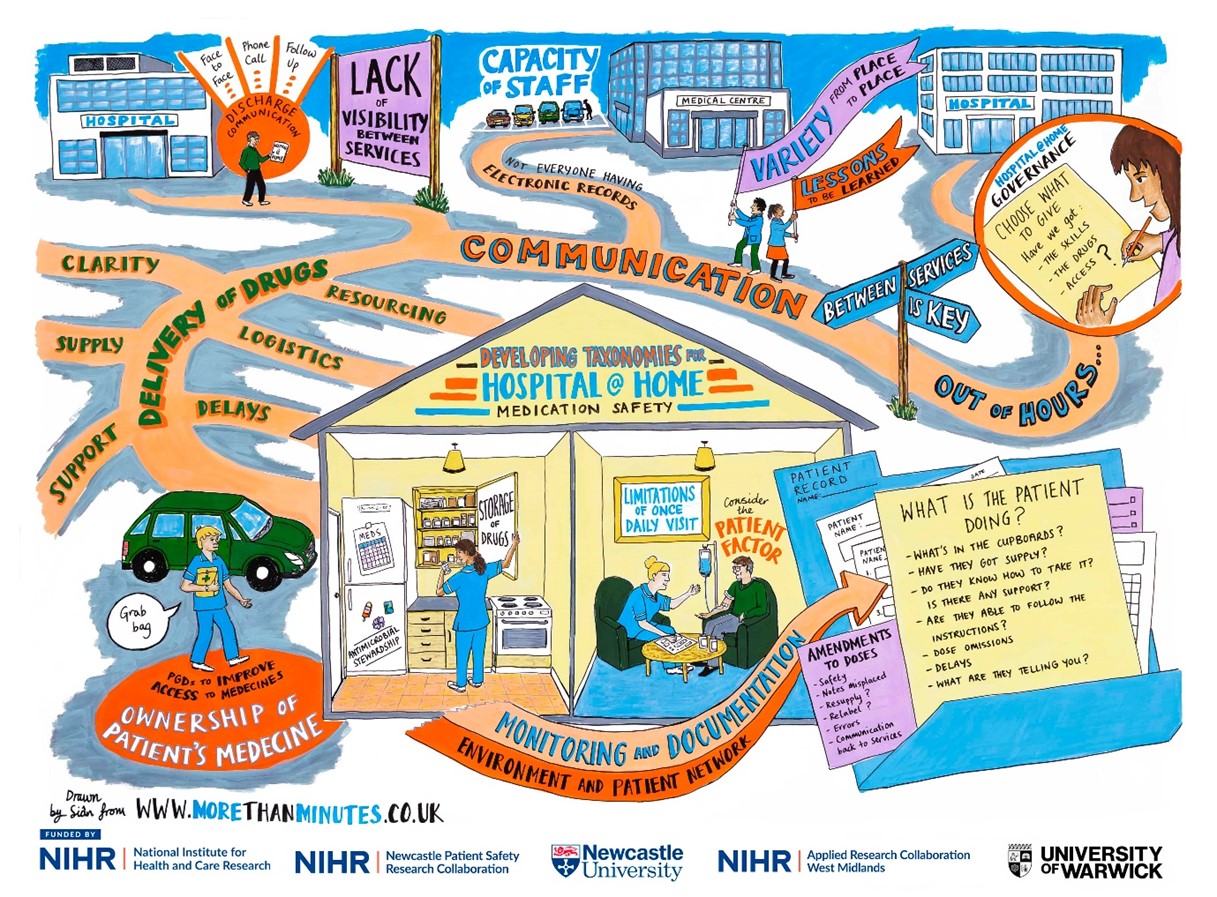
Figure 1 above
How it all began?
I remember attending my first Hospital at Home Society conference in 2024. At this point, I was in the early days of the PhD, eager to learn more about current developments in this research area. During the networking breaks, I remember introducing myself to keynote speakers and little did I know that this would be the start of a wonderful collaboration and supervision for the NIHR SPARC Award.
I was keen to discuss the priority research areas for Hospital at Home (H@H) and later that year, I came across the NIHR SPARC Short Placement Award for Research Collaboration | NIHR. I felt that this was a wonderful opportunity to work with a research team that had the expertise in H@H, who operationally had the research knowledge, the technical and practical expertise in this field, and the existing networks that I could learn from and engage with moving forward. Additionally, my aspirations for professional development to become a clinical academic drove my passion to work with a group of dedicated and trailblazing clinical academics. I felt this would strengthen my experience, especially when considering post-doctoral opportunities.
What is the SPARC award for?
The NIHR SPARC Award allows NIHR academy members to spend time with researchers across other NIHR infrastructure to enhance their personal and professional development and research training experience. From speaking to previous candidates, I learned that this is usually either to develop skills in particular research methods, or to develop collaborations and expertise from researchers in a particular field.
What I did?
The application itself allows you to be quite flexible in how you undertake the placement, which is helpful depending on what you want to achieve. Personally, I had set out 1 day a week over 9 months, whereas other previous applicants undertook it in block placements (e.g. in a 4-week block).
During the placement I managed to conduct clinical visits to H@H services to get the first-hand practical experience. I attended clinical meetings and research meetings linking in with other health tech research centres in the NIHR infrastructure. As part of the award, I also accounted for attending courses and conferences around implementation science and knowledge mobilisation which I felt would be useful for my professional development and demonstrating meaningful impacts with research. The bulk of the collaborative work centred around working on a multi-phase research project. This involved a literature review and arranging an online stakeholder workshop with clinical experts nationally to discuss the findings. This also involved working with a visual minutes artist and presenting the findings at the UK Hospital at Home Society Conference 2026, at the Royal College of Physicians in Edinburgh, which supported input into the survey with H@H practitioners.
Outputs of the placement?
This placement allowed us to develop a Taxonomy of Medicines Safety in Hospital at Home which is aimed for upcoming publication. This enables a better understanding of the concepts of medicines safety in H@H and the links between them. Although the aim of the placement is professional development, I was fortunate to have an abstract accepted for oral presentation at the UK Hospital at Home Society conference in 2026, which is planned for submission to the Journal of Advanced Home Medicine. Additionally, a visual minutes graphic produced from this work is displayed below (See Figure 1).

Blog produced by Faiza Yahya (PhD Candidate), with acknowledgements to the support and supervisory team at the University of Warwick (Professor Daniel Lasserson, Dr Ciara Harris, Sophie McGlen) and the NIHR for funding this award. Appreciation also goes to the Academic Career Development Leads (Newcastle University and NIHR ARC West Midlands) for making this happen.
with Francesca Morland

11.30 – 12.30. Howden Room, King George VI building
VCSE Research Partnerships at VONNE
“Working with the Voluntary, Community and Social Enterprise (VCSE) sector in health and care research- VCSE Research Partnerships at VONNE”
Francesca Morland is VCSE Research Partnerships Coordinator at Voluntary Organisations’ Network North East (VONNE). Her role focusses on bringing together the Voluntary, Community and Social Enterprise (VCSE) sector and health and care research sectors, to form more reciprocal and sustainable partnerships.
This session will focus on with the VCSE sector is and how they can be a valuable partner in research. It will include an overview of the VCSE landscape in the region, what they can offer to health research and how to engage effectively with communities through the VCSE sector. Fran will also present what support is available to researchers through VONNE when connecting with communities.
Register by scanning the QR code below or clicking the register here link below.

Pippa Wood NIHR Newcastle PSRC Operations Manager
I went to the NIHR SafetyNet Organisational Culture working group meeting in Birmingham on a cold day in January. I wanted to learn what “organisational culture” means and how it links to patient safety.
So, what is organisational culture?
After listening to researchers from different PSRCs, I learned that organisational culture is basically how people at work get along. It includes the relationships between colleagues, managers, departments, services and different job roles.
How does this affect patient safety?
The way people treat each other at work can directly affect the care patients receive. If communication and relationships between teams are poor, things can go wrong.
For example:
- A patient might be sent home from hospital, but no one tells their family or carers, so no one is there to meet them.
- A family may still be waiting for a call to say they can collect their loved one, only to find out the patient has already been taken home by hospital transport.
But when communication and teamwork are good, patients get much better care.
For example:
- Maternity staff might tell new mothers about breastfeeding support available in their community.
- If an older person is having surgery, hospital staff may work with community care teams and family members to plan what help the patient will need at home.
The biggest thing I learned
If staff are unhappy, feel unappreciated, experience bullied, or feel insecure in their jobs, this can lead to poor communication and bad relationships at work. This can then cause poor-quality services, lower standards of care, and higher risks to patient safety.
But if staff feel happy, valued, and supported, they are more likely to work well together. Good relationships between teams mean better services, higher standards of care, and safer experiences for patients.

Dr Matthew Cooper, NIHR Newcastle PSRC Safer Integrated Health and Social Care Environments, Research Associate
Dr Matthew Cooper, NIHR Newcastle PSRC Safer Integrated Health and Social Care Environments, Research Associate
Broadening My Understanding of Organisational Culture
Attending the organisational culture working group helped me to broaden my understanding of what organisational culture truly represents. Initially, I viewed workplace culture mainly in terms of supporting staff wellbeing and keeping people happy and healthy at work. Through the discussions, I realised how strongly organisational culture also influences patient safety and the consistent delivery of high-quality care.
Exploring the Ambition of the 10‑Year Plan
The working group explored the ambition of the 10-year plan, which is expected to drive change both during the next 10 years and for the future beyond. This however highlights some key risks:
- That pressure to deliver quickly could lead to rushed decisions,
- Missed input from some disciplines (implementation science for example), or
- Action being taken without full consideration of the plausible impacts (for example removing resources from one service to fund a new idea).
A strong emphasis was placed on transparency of quality of care, including empowering patients through greater voice, choice and access to information. This was balanced alongside clearer accountability and stronger incentives for high-quality care. I was particularly struck by the challenge of double running costs, where services must continue to operate while resources are reallocated, and the importance of deliberately creating time for safety within this context.
Reaffirming the Core Purpose of Organisational Culture
Overall, the working group reinforced that the core goal of organisational culture is to support patients, underpinned by robust checks and balances, compassionate leadership, and a shared commitment to quality and safety at every level of the system. As a team at the NIHR Newcastle PSRC, this is something we are all hoping to reflect on and take forward in our research.
Learn more about the NIHR 10 year plan.
by Nathania Bestwick NIHR Newcastle PSRC PhD student
I was grateful to travel to London for the PSYCH Symposium 2025 on Thursday, 4th December. This symposium brings together researchers, therapists, doctors, policymakers, investors, and campaigners to talk about the latest research in psychedelic medicine and how psychedelic therapies may be used in mainstream healthcare to treat mental health conditions.
I attended the symposium with Radin Karimi, another PhD student from the NIHR Newcastle Patient Safety Research Collaboration (PSRC). Like my own work, Radin’s research looks at how to better manage polypharmacy (which is when people take many different medicines at the same time). Medicines used to treat mental health conditions often add to this problem, so we were interested to find out if psychedelic therapies might help people manage their mental health so they can take fewer medicines. We were also keen to learn how patient safety is managed in this developing area of research.

The symposium focused on a range of conditions, including depression, anxiety, PTSD, addiction, eating disorders and distress near the end of life, particularly for people who have not responded to more commonly used treatments. Speakers shared evidence showing that psychedelic medicine, such as psilocybin, MDMA and ibogaine, can help to ease symptoms in people with these conditions. They also explained that psychedelic therapies may help people process deeper emotional problems behind their symptoms, which can lead to longer-lasting improvements in well-being. Several speakers had worked with military veterans and shared how these therapies have helped them manage PTSD, support their mental health, and feel better in everyday life after leaving the military.
Patient safety was a major focus throughout the symposium. Research in this area is strictly regulated, with people being carefully checked (called screening) before they’re invited to take part, and with study information being clearly explained so that people can make an informed choice when agreeing to join a study. Therapies are provided in carefully controlled and supportive treatment spaces by highly trained therapists and healthcare professionals, with close monitoring during sessions, and follow-up support after the treatment to help people understand their experiences and get the best results from the treatment.

Professors David Nutt and Guy Goodwin had an interesting discussion about recent results from a large study which showed that a single dose of synthetic psilocybin helped people with severe, long-lasting depression, with higher doses leading to bigger improvements in symptoms. They also spoke about drug laws creating stigma around psychedelic research, even though there is growing evidence that these substances can have real health benefits and that they may be less harmful than legal drugs, such as alcohol and tobacco.
One example of how psychedelic medicine is being used in standard healthcare came from Professor Ranil Gunewardene, who described how he is leading one of the first clinics in Australia to offer regulated psychedelic-assisted therapy. Since his research is with patients who have complex health conditions (called real-world patients), it may give us helpful insight into how these therapies can be used outside of highly controlled research environments.
In summary, the symposium showed that psychedelic medicine has promising potential to improve care for people with mental health conditions, particularly those that are difficult to treat. It also highlighted that more research is needed and that building upon the current evidence base will help us better understand how effective and safe these treatments are, and how they can be carefully and appropriately used as part of standard healthcare.
Details and bios for each of the speakers can be found here
Yahya F, Cooper M, Saif W, Kassem M, Nazar H Development of a Hospital at Home Digital Twin for Patients With Frailty: Scoping Review Journal of Medical Internet Research 2025;0:e0 URL: https://www.jmir.org/2025/1/e81510 doi: 10.2196/81510
What’s this about?
How can we make the most of advanced technology and live information to improve how we deliver hospital-level care at home?

What’s this about?
How can we make the most of advanced technology and live information to improve how we deliver hospital-level care at home?
Why are we looking at this?
The NHS 10-year plan wants to:
- Move more care from hospitals closer to home
- Prevent illness instead of just treating it
- Use more digital tools to support care

What is the work we are doing?
We explore all three by using something called Digital Twins. A Digital Twin is like a live virtual simulation of a patient and their surroundings using real-time information. It can help healthcare professionals predict problems early, to give care that’s safer and more personalised.
Learning from, and working with other experts, our work looked at creating a simple step-by-step model, which can be used to develop a Hospital-at-Home Digital Twin. This review was based on existing evidence for tools to support this, for patients living at home with frailty.
What does this mean?
- Technology and real-time data can help health professionals care for patients at home more efficiently.
- Digital Twins could make care timelier, safer, and tailored to each person.
- We’ve outlined the main building blocks for creating a Hospital at Home Digital Twin.
This work is just the beginning, but it shows how technology could possibly change the world of healthcare and what needs to be worked on to make this possible.
For those that want to know more:
Our article reviews the current evidence for tools that exist to support the development of a Hospital at Home Digital Twin. We describe the 5 layers required to build a Digital Twin. Results show that a variety of technologies exist to pick up information, such as wearables. However more understanding is needed of how we manage that data, store it, translate it and use it to make useful predictions to help staff who are looking after us make decisions. This article also talks about some of the challenges and opportunities we may face when using these technologies in our current healthcare system.
By Kamil, NIHR Newcastle PSRC Patient, Public Contributor
Lured by the promise of good food and new acquaintances, on Friday 17 October I made my way to Manchester for the NIHR SafetyNet Symposium – a gathering of clinicians, researchers and public contributors united by a single mission: tackling inequities in patient safety. Hosted by the Greater Manchester Patient Safety Research Collaboration (PSRC), the event brought together colleagues from the six PSRCs across England – Central London, Greater Manchester, Midlands, Newcastle, North West London and Yorkshire & Humber.
The day began with coffee and a bustling lobby filled with poster presentations. From the start, it was clear this wasn’t just an academic exercise. It was a collective effort to bridge the gap between policy, practice and lived experience.
One of the first things that struck me was the keynote by Dr Rosie Benneyworth from the Health Services Safety Investigations Body (HSSIB). I hadn’t heard of HSSIB before and I found its mission fascinating. The organisation investigates systemic issues in healthcare topics such as sepsis, prison health and fatigue without focusing on blame. Instead, it looks for learning and improvement. This shift from a ‘who’s to blame’ culture to one of collective accountability resonated deeply with me.
A presentation on avoidable healthcare-associated harm in prisons was another eye-opener. While I wasn’t surprised to hear that prisoners and people experiencing homelessness suffer significantly worse health outcomes, it was sobering to see how these inequities manifest in daily practice e.g. medication shortages, missed appointments and institutional barriers that make basic care difficult. As someone finishing reading a book on health promotion, I could connect the dots between theory and reality: these are not abstract inequalities, they are lived injustices.

One reflection that stayed with me came from a discussion about adoption and breaking cycles of poverty and violence. Even in systems that often feel broken, there are ways to create safety and opportunity through compassion and action.

Several sessions focused on the intersection of communication and safety, including translation and interpreting services. This hit particularly close to home. As a qualified Polish interpreter, I know how vital accurate translation is for patient safety, yet the pay rates offered by NHS providers are often so low that professionals can’t afford to take the work. Hearing that language access was being discussed as a safety issue, not just a convenience, was both encouraging and frustrating. We have the knowledge; now the system needs the will to act.
The Patient Safety Healthcare Inequalities Reduction Framework, presented by Dr Hester Wain, outlined five principles for change: communication and information, training and resources, data, co-production, and research. I was especially struck by her emphasis that the experiences informing the framework are what make it powerful.
By the end of the day, after many conversations in the poster corridor and a moving talk on ethnic inequities in patient safety by Professor Dawn Edge, I left Manchester feeling both hopeful and challenged. The message was clear: health doesn’t happen in a vacuum. Tackling inequity requires empathy, collaboration, and, above all, a commitment to listen to those whose voices are too often ignored. For me, as a patient-cum-public contributor, the symposium was a reminder that my lived experience isn’t just welcome in research – it’s essential.
By Dr Anna Robinson-Barella and Dr Matt Cooper
Along with several of our NIHR Newcastle PSRC colleagues, Matt and I attended the SafetyNet symposium on Friday 17th October in Manchester. The focus of the event was: “Tackling Inequalities in Patient Safety”. It was a day that encouraged a lot of reflection-primarily upon patient safety and our cross-PSRC SafetyNet-agenda, but also upon intersectional influences including ethnicity, marginalisation, and wider EDI-related issues underpinning our work.
We heard from speakers across all six of the PSRCs, as well as two keynote speakers, Dr Rosie Benneyworth presenting “Moving away from a “whose to blame” culture” and Prof Dawn Edge presenting “Ethnic Inequalities in Patient Safety”.
NIHR Newcastle PSRC had 32 of our colleagues in attendance; many of whom presented research posters about their work covering topics like polypharmacy, medicines adherence, costs and treatment decisions, social prescribing, health-related quality of life, and predicting diseases by using AI.
It was also a pleasure to personally contribute to the agenda of the day, and represent NIHR Newcastle PSRC, by presenting an evidence synthesis on inequities affecting medicines access for people experiencing homelessness and the subsequent consequences on their (patient) safety.
Congratulations to all the team involved in organising, hosting and running a great symposium!


By Henry Song, Artificial intelligence and data science in multiple long-term conditions theme PhD student
Attending the NIHR Newcastle PSRC/Pharmacy event on the 19th of June was a very positive experience for me. Although I was not able to present my latest research findings due to recent changes in my project dataset, the day still proved to be highly valuable.
I had the chance to see a wide range of presentations from fellow students and colleagues. Some of the work provided direct inspiration for my own research, while others helped to broaden my perspective on the diverse approaches within our field. I was particularly struck by the experimental-based studies on display, which were not only highly innovative but also showed real potential for future impact.
In the afternoon, the workshop on research funding applications was especially useful. It gave me a first insight into the key steps, structure, and approaches involved in applying for research grants. This will no doubt be very important as I continue to develop my academic career.
Overall, the event was an excellent opportunity to learn, connect, and reflect on both my own project and the wider research landscape.
Experience of participation and poster presentation.
By PhD Student Rajeev Shrestha
On 18th July 2025, I got the opportunity to attend the Great North Pharmacy Research Collaborative (GNPRC) Conference, held at the Hilton Hotel, Gateshead. This event brought together pharmacy professionals, researchers, and pharmacy trainees to explore innovations in medicines optimisation, collaboration, and workforce development.
A key highlight for me was presenting my poster titled “Outcome of Deprescribing in People with Life-Limiting Conditions: A Systematic Review”. This study aimed to synthesise evidence on the clinical-, medicine and system-related outcomes of deprescribing practices among palliative patients. I had an opportunity to interact with fellow attendees during the poster viewing sessions that really sparked meaningful conversations around the safer use of medication. Personally, it was encouraging to see the ongoing works on reducing inappropriate use of medication by practising pharmacists.
The conference agenda was rich with insightful sessions. I particularly appreciated the breakout session on “Shared Decision Making and its Role in Reducing Overprescribing,” which also resonate with the area of my research. The growing emphasis on collaboration across sectors, from community pharmacies to NHS manufacturing, highlighted the evolving role of pharmacists in shaping safer, more effective care pathways.
Overall, GNPRC 2025 was a valuable experience to me. The event inspired new ideas, informed ongoing initiatives and deepened our commitment to contributing to quality use of medications.
I’m Liam, a Specialist Clinical Pharmacist in Acute and Emergency Care at Northumbria Healthcare NHS Foundation Trust. I split my time between clinical practice (four days a week) and research (one day a week) through the NIHR Newcastle PSRC Patient Safety Development Award. Since graduating from Newcastle University’s School of Pharmacy in 2022, I’ve been building my research career alongside clinical development, driven by a passion for research sparked during my undergraduate studies.

The NIHR Newcastle PSRC’s impact on clinicians
Traditionally, clinical practice and academia have been seen as separate career paths. Clinicians interested in research often had to pursue it in their own time, outside of demanding full-time roles.
The NIHR clinical academic pathway has transformed this by funding protected research time and reimbursing employers, allowing clinicians to step away from practice to pursue research.
For me, this has meant one day each week seconded at NIHR Newcastle PSRC, where I’ve developed core research skills. Working with experienced researchers has helped me understand the full project lifecycle, from shaping early ideas and designing methodology to recruiting participants, collecting data, and writing up results.
Building Collaborations
Embedding clinicians within the NIHR Newcastle PSRC helps build strong links with partner organisations. Connections with charities and local health and social care providers create future opportunities at both individual and organisational levels. This also broadens the chance for under-represented groups to have a voice, influence practice, and help reduce health inequalities.
At Newcastle University, embedded clinicians benefit from access to leading academics in their field and can learn from their experience. Previously, collaborations were often ad hoc, such as draft reviews or methodology advice. These awards now enable clinicians to work more closely with academics and gain a deeper understanding of research and academia.
Why is this valuable to the public?
Research-active organisations are linked to better patient outcomes. Combining clinical work with research lets me address real issues I encounter in practice, shaping projects that can drive meaningful change.
In acute medicine, I’ve focused on discharge and follow-up challenges. Through the NIHR Newcastle PSRC, I’m now working on a project exploring these issues for homecare recipients and those working in the industry.
Being embedded in both sectors also helps spread research findings more effectively, supporting better service improvements and outcomes.
Next Steps
A key goal is to encourage more healthcare professionals to engage in research. The NIHR clinical academic pathway supports this by offering development alongside clinical roles, leading to qualifications and national research leadership opportunities.