Click below to register
Register here
To mark Deaf Awareness Week 2026, our Director of EDI worked with students at the Newcastle School of Pharmacy to create a short blog about D/deaf awareness, inclusive pharmacy care and how this relates, in an actionable way, to patient safety.
The theme for this year’s Deaf Awareness Week was, ‘Right to understand – Together, we break barriers.’ This theme aimed to raise awareness for the communication needs of the D/deaf community and advocate for greater access to communication tools and services to support safe and inclusive consultations with patients.
Pharmacists and pharmacy teams play a key role in creating a safe space to support members of the Deaf community and ensuring equitable access to medication services. We can do this by educating ourselves on basic sign language, maintaining face-to-face contact, utilising visual/written aids and remaining open to conversation.
“Adaptation is a constant part of my life… the solutions to help bridge the gap are versatile and very much individualised” – Annissa Wiltshire, MPharm student and member of the Deaf community
Newcastle University’s BSL workshop is a great example of how we can undergo further training to educate ourselves. Newcastle Alumni and Foundation Trainee Pharmacist, Christina Newell, found the BSL training be “invaluable” in informing her work: “[doing BSL] pushed me to be a better healthcare professional with patients and carers who use this language to communicate. It also helped me develop different skills, such as being patient, knowing how to communicate with others using my body language and how to be focused and attentive to somebody when communicating with them.”
In pharmacy practice, ensuring information is clear, adaptable, and responsive to individual needs is essential to delivering safe, person-centred care and reducing health inequalities.
Blog post written by: Melika Ghazi-Nouri, Annissa Wiltshire, and Cristina Newell.

What can we learn from someone who has spent more than thirty years navigating complex health challenges? As This Curious Life begins its Global Conversation on Multiple Health Conditions, Victoria Bartle’s story offers a powerful reminder that some of the most important expertise in healthcare does not always come from textbooks, research papers or data. Sometimes it comes from the people living the reality every day.
At the NIHR Newcastle PSRC, we are dedicated to improving safety and care for people living with multiple long-term conditions. While our research relies on rigorous scientific frameworks, Victoria’s insights highlight exactly why data alone isn’t enough. True progress happens when we combine clinical data with the deep, practical wisdom of patients who manage these complexities every single day.
Victoria’s journey shines a light on the questions that spreadsheets simply cannot answer—and reminds us who we are ultimately innovating for.
We invite you to dive into this insightful piece, explore the realities of navigating long-term conditions, and join the global conversation:
The Question Data Couldn’t Answer – This Curious Life

Victoria Bartle
This Dementia Action Week, we shared examples of education and research efforts led by people in our PSRC…

First up: Dr Anna Robinson-Barella, our Director of EDI in the PSRC, recently collaborated with colleagues at NIHR Join Dementia Research to film a short series about how pharmacists can support people impacted by Dementia (including patients and their carers/friends/family members). 💙🌼🎥
Anna interviewed Sarah, who spoke about her experiences being a carer for her Mam, who was living with dementia. She discussed ways that pharmacists and wider members of the pharmacy team can support those impacted by dementia and the videos complemented teaching for teaching on the Master of Pharmacy degree at Newcastle University.
This work was supported by Anna’s collaborators: Dan Duhrin, Nichol Quinn and Lisa Duggan-Howarth at NIHR JDR.

Next: is work done by PSRC PhD researcher, Lauren Lawson, and her supervisory team (Dr Matt Cooper, Dr Clare Tolley, Prof Annette Hand and Prof Hamde Nazar). Lauren’s second publication from her PhD is titled “There doesn’t seem to be the help there for people who are carers”: Qualitative findings from a realist evaluation of hospital-to-home transitions. 💙
Read it here: https://academic.oup.com/innovateage/advance-article/doi/10.1093/geroni/igag056/8687114?login=true.
Lauren’s study looked at the experiences of unpaid carers supporting older adults with dementia and long-term conditions, when moving from hospital back home. 🏥
Findings suggested that many carers felt overwhelmed, unsupported, and unsure where to turn for reliable information, highlighting the need for clearer communication and more personalised support when someone with dementia and long-term conditions leaves hospital.

I am delighted to introduce myself as a new Clinical Research Fellow in Patient Safety and a member of the Academic Career Development (ACD) team here at the NIHR Newcastle PSRC. Joining the NIHR Newcastle PSRC is a fantastic privilege and something that I fully intend to make the most of. This opportunity feels like a natural next step in my research journey that has always been focused on making healthcare work better for the people who need it most.
My Background:
I am a Physiotherapist by background and am starting this position as a secondment from my NHS Trust – Tees, Esk and Wear Valleys NHS Foundation Trust (TEWV). My clinical career to-date has covered both in patient and community physical health settings, before a transition to working specifically within inpatient mental health settings for working age adults.
In these roles, I saw first-hand how complex the intersection of physical and mental health can be. It became clear to me that patients with severe mental illness (i.e. psychosis, schizophrenia, schizoaffective disorder, or bipolar disorder) often face many difficulties, not just from their primary diagnosis, but from the challenges of managing their physical health within a mental health setting. This is one of the areas that I hope to improve through my own research.
My Research Journey:
My introduction to clinical research was via a 9-month NIHR internship, leading to a 2-year part-time NIHR Pre-doctoral Clinical Academic Fellowship (PCAF). Following this I began my PhD part-time alongside my clinical work via a partnership between TEWV and York St John University.
My PhD has involved focusing on the complex relationship between physical symptoms (such as walking and daily functioning) and psychological symptoms (specifically anxiety and depression) in people living with Parkinson’s. This work has involved considering the perspectives of people living with Parkinson’s, their carers, and UK-based physiotherapists, alongside cross-sectional and longitudinal analysis of various physical and psychological assessments. I am approaching the end of my PhD and alongside preparing to submit, I am in the process of developing some recommendations for clinical practice.
My other research interests focus on promoting sustainable long-term lifestyle and behaviour change to improve both physical and mental wellbeing. I am particularly interested in how we can move beyond short-term interventions to create lasting habits that improve quality of life. In the context of patient safety, this means looking at how health behaviours, such as physical activity and self-management, can act as a safety net, reducing the risk of secondary complications and hospital readmissions for those with complex needs.
Looking Forward:
At the NIHR Newcastle PSRC, I’ll be wearing two hats that I’m equally passionate about:
- In Academic Career Development (ACD): I know how daunting the clinical academic path can feel. Having navigated my pre-doctoral and (almost!) doctoral routes, I am excited to support others in finding their own routes into research. To me this will focus on individual development alongside supporting impactful research.
- In Patient Safety: I’ll be applying my clinical experience to help recognise risks and improve safety, particularly for populations that often fall through the cracks of traditional healthcare systems. For example, I have recently been successful in obtaining NIHR Three School Prevention funding. This will fund the PATHS to prevention project to explore current provision of physical activity support during the transition between inpatient and community mental health settings. We hope to build on the findings of this work to co-design improved pathways for maximising long-term engagement with physical activity to help both physical and mental health.
Let’s Connect:
The best research happens when we work together. Whether you’re a clinician with a nagging research question or a fellow researcher interested in mental health safety, I’d love to chat. I’m new to the PSRC and Newcastle University so I’d also love to connect with other colleagues with similar research interests.
You can find more details about my publications on ResearchGate or read more about my personal journey via Routes to Research.
My usual working days within the PSRC will be Wednesday-Friday.
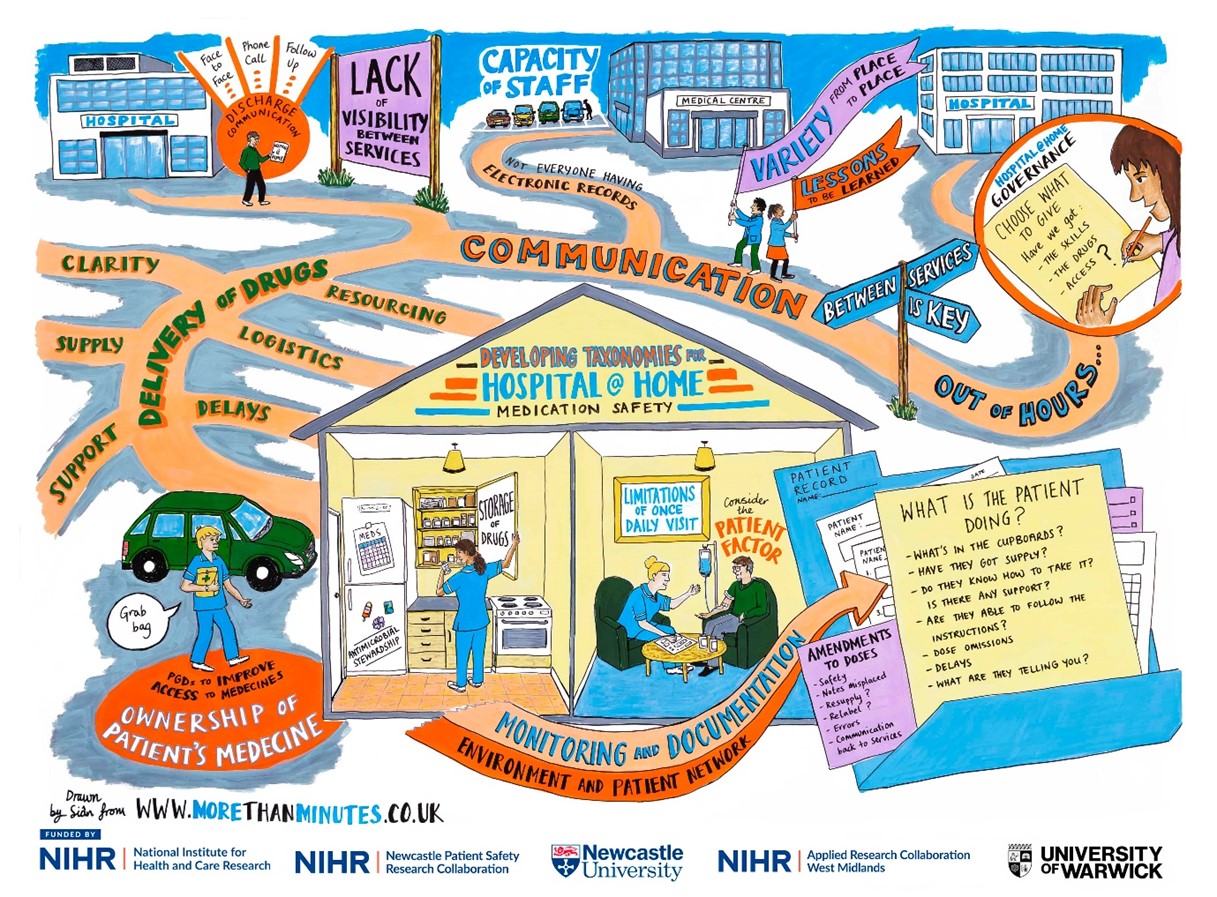
Figure 1 above
How it all began?
I remember attending my first Hospital at Home Society conference in 2024. At this point, I was in the early days of the PhD, eager to learn more about current developments in this research area. During the networking breaks, I remember introducing myself to keynote speakers and little did I know that this would be the start of a wonderful collaboration and supervision for the NIHR SPARC Award.
I was keen to discuss the priority research areas for Hospital at Home (H@H) and later that year, I came across the NIHR SPARC Short Placement Award for Research Collaboration | NIHR. I felt that this was a wonderful opportunity to work with a research team that had the expertise in H@H, who operationally had the research knowledge, the technical and practical expertise in this field, and the existing networks that I could learn from and engage with moving forward. Additionally, my aspirations for professional development to become a clinical academic drove my passion to work with a group of dedicated and trailblazing clinical academics. I felt this would strengthen my experience, especially when considering post-doctoral opportunities.
What is the SPARC award for?
The NIHR SPARC Award allows NIHR academy members to spend time with researchers across other NIHR infrastructure to enhance their personal and professional development and research training experience. From speaking to previous candidates, I learned that this is usually either to develop skills in particular research methods, or to develop collaborations and expertise from researchers in a particular field.
What I did?
The application itself allows you to be quite flexible in how you undertake the placement, which is helpful depending on what you want to achieve. Personally, I had set out 1 day a week over 9 months, whereas other previous applicants undertook it in block placements (e.g. in a 4-week block).
During the placement I managed to conduct clinical visits to H@H services to get the first-hand practical experience. I attended clinical meetings and research meetings linking in with other health tech research centres in the NIHR infrastructure. As part of the award, I also accounted for attending courses and conferences around implementation science and knowledge mobilisation which I felt would be useful for my professional development and demonstrating meaningful impacts with research. The bulk of the collaborative work centred around working on a multi-phase research project. This involved a literature review and arranging an online stakeholder workshop with clinical experts nationally to discuss the findings. This also involved working with a visual minutes artist and presenting the findings at the UK Hospital at Home Society Conference 2026, at the Royal College of Physicians in Edinburgh, which supported input into the survey with H@H practitioners.
Outputs of the placement?
This placement allowed us to develop a Taxonomy of Medicines Safety in Hospital at Home which is aimed for upcoming publication. This enables a better understanding of the concepts of medicines safety in H@H and the links between them. Although the aim of the placement is professional development, I was fortunate to have an abstract accepted for oral presentation at the UK Hospital at Home Society conference in 2026, which is planned for submission to the Journal of Advanced Home Medicine. Additionally, a visual minutes graphic produced from this work is displayed below (See Figure 1).

Blog produced by Faiza Yahya (PhD Candidate), with acknowledgements to the support and supervisory team at the University of Warwick (Professor Daniel Lasserson, Dr Ciara Harris, Sophie McGlen) and the NIHR for funding this award. Appreciation also goes to the Academic Career Development Leads (Newcastle University and NIHR ARC West Midlands) for making this happen.
When “help” might harm: understanding the safety of social prescribing
Social prescribing has become a cornerstone of person-centred care, connecting people to community support, reducing pressure on services, and improving wellbeing. But what happens when these interventions don’t go as planned?
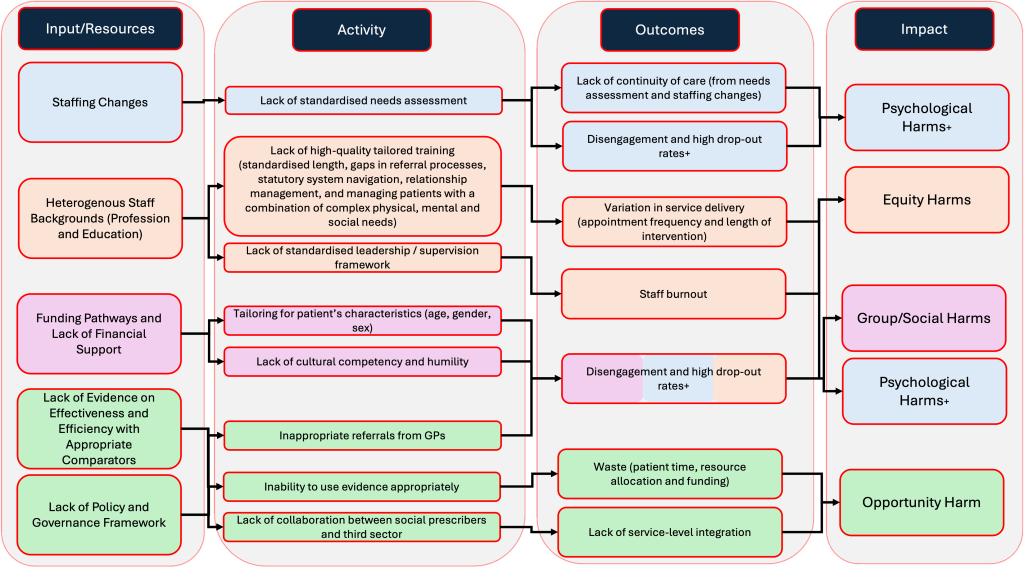
In our recent study, we looked beyond effectiveness to explore an underexamined issue: the potential harms of social prescribing. Using a global umbrella review of existing evidence, we developed a “dark logic” model (a way of mapping how unintended negative consequences might arise).
What did we find?
While social prescribing can offer important benefits, the evidence base highlights several areas of potential risk:
- Mismatch between needs and services – when referrals don’t align with individual circumstances, leading to frustration or disengagement
- Equity concerns – where access to community resources is uneven, potentially widening inequalities
- Burden transfer – shifting responsibility onto individuals or overstretched voluntary sector services
- Psychological impacts – including feelings of stigma, rejection, or failure if support pathways break down
Importantly, many of these harms are not the result of single decisions, but emerge through complex systems of care, commissioning, and delivery.
Why this matters for patient safety
Patient safety conversations have traditionally focused on clinical interventions. Our findings suggest we need to extend that thinking into community-based and non-medical models of care.
Social prescribing operates across organisational boundaries (primary care, local authorities, and the voluntary sector) which can create gaps in oversight, accountability, and follow-up. Without careful design, implementation, and evaluation, there is a risk that well-intentioned interventions could inadvertently contribute to harm.
What can we do differently?
Our “dark logic” model is not about discouraging social prescribing, but about making it safer and more equitable. Key implications include:
- Building safety considerations into service design from the outset
- Strengthening monitoring of outcomes beyond uptake and satisfaction
- Supporting the voluntary and community sector to deliver sustainable services
- Ensuring equity is a central focus in referral pathways and access
- Recognising and addressing the emotional and psychological experiences of participants
Looking ahead
As social prescribing continues to grow, there is an important opportunity to embed patient safety principles into its development. This means moving beyond asking “does it work?” to also asking “for whom, in what contexts, and at what cost?”
By bringing a safety lens to this evolving area of practice, we can better ensure that social prescribing delivers on its promise, without leaving unintended harms unseen.
Call to action
We encourage researchers, practitioners, commissioners, and community partners to actively incorporate safety thinking into social prescribing policy and practice. This includes:
- Designing services with potential harms in mind, not just intended benefits
- Sharing learning on unintended consequences across organisations and sectors
- Embedding routine monitoring of safety outcomes in evaluation frameworks
- Involving patients and communities in identifying what “safe” support looks like in practice
By working collaboratively and proactively, we can ensure that social prescribing not only supports wellbeing, but does so safely, equitably, and sustainably.
Paper link – https://bmjopen.bmj.com/content/16/5/e108998.abstract
Perspectives from the PSRC Newcastle, Disadvantaged Communities Theme were included in a new report from Bowel Cancer UK on cancer diagnoses in hospital emergency departments – which is the foundation of a new campaign by the charity on this topic.
This patient insight report is an important first step in understanding the experiences of people and families affected by emergency bowel cancer diagnoses. Hearing these perspectives helps us appreciate the emotional and practical impact on patients and their loved ones, while also beginning to identify areas where improvements could make a real difference.
Connecting experiences from both patients and professional viewpoints helps us develop a complete picture of what happens, what is working and what may need to change. This comprehensive understanding is the first step in making sure that future interventions are grounded in real experiences and, ultimately, that patients and families are better supported.
Please follow the link below to read the full report:

Wednesday 16th September 09:30-16:30, Urban Sciences Building, Newcastle Helix, NE4 5TG

How do we make healthcare safer, fairer, and more connected for everyone?
Join the NIHR Newcastle Patient Safety Research Collaboration (PSRC) for an inspiring day dedicated to showcasing the groundbreaking research and projects we have driven forward over the last four years.
This showcase is a unique opportunity to explore how our research is directly improving patient safety, hear first hand how Patient and Public Involvement and Engagement (PPIE) is at the heart of everything we do, and connect with the minds behind the science.
Why Attend?
- Join Rachel Carter, Director of Quality & Safety and Patient Safety Specialist at Newcastle upon Tyne Hospitals NHS Trust, as she discusses the key patient safety challenges facing large NHS trusts in 2026. Rachel will explore the Trust’s strategic priorities, the drivers shaping its safety agenda, and her perspective on the future direction of patient safety across the organisation.
- Explore Our 4 Core Themes: Dive deep into the four pillars of our research:
Polypharmacy: Safer management of polypharmacy in multiple long-term conditions
Disadvantaged Communities: Safer management of multiple long term conditions in disadvantaged communities
Data and AI: Artificial intelligence and data science in multiple long-term conditions
Integrated Health and Social Care: Safer integrated health and social care environments
- Engage in the Conversation: Each theme will feature a series of rapid-fire project presentations followed by a live, interactive panel discussion. We want to hear your voice—bring your questions and join the debate!
- See PPIE in Action: Discover how patients and the public have actively co-designed and shaped our research to ensure it addresses real-world needs.
- Network & Connect: Visit our interactive theme stands during breaks. It’s the perfect space to chat informally with researchers, view project posters, and build valuable collaborations.
Who Is This Event For?
This event is free and open to everyone interested in the future of healthcare safety, including:
- Healthcare and social care professionals
- Researchers, academics, and students
- Patients, public contributors, and community advocates
- Policy makers and industry partners
Spaces are limited, so reserve your free ticket today and help us shape the future of patient safety!
Register Now on Eventbrite at the button below
For any inquiries regarding accessibility or dietary requirements, please contact PSRC@newcastle.ac.uk
The next Newcastle School of Pharmacy EDI Event is taking place on Wednesday the 18th of March 2026 from 12.00 in the DENT RBG Lecture Theatre, Medical School, Newcastle University.
Register your interst by emiling: Anna Robinson-Barella, Director of EDI:
anna.robinson-barella@newcastle.ac.uk
@NCL_Pharmacy
@FMSdiversityNCL

Pippa Wood NIHR Newcastle PSRC Operations Manager
I went to the NIHR SafetyNet Organisational Culture working group meeting in Birmingham on a cold day in January. I wanted to learn what “organisational culture” means and how it links to patient safety.
So, what is organisational culture?
After listening to researchers from different PSRCs, I learned that organisational culture is basically how people at work get along. It includes the relationships between colleagues, managers, departments, services and different job roles.
How does this affect patient safety?
The way people treat each other at work can directly affect the care patients receive. If communication and relationships between teams are poor, things can go wrong.
For example:
- A patient might be sent home from hospital, but no one tells their family or carers, so no one is there to meet them.
- A family may still be waiting for a call to say they can collect their loved one, only to find out the patient has already been taken home by hospital transport.
But when communication and teamwork are good, patients get much better care.
For example:
- Maternity staff might tell new mothers about breastfeeding support available in their community.
- If an older person is having surgery, hospital staff may work with community care teams and family members to plan what help the patient will need at home.
The biggest thing I learned
If staff are unhappy, feel unappreciated, experience bullied, or feel insecure in their jobs, this can lead to poor communication and bad relationships at work. This can then cause poor-quality services, lower standards of care, and higher risks to patient safety.
But if staff feel happy, valued, and supported, they are more likely to work well together. Good relationships between teams mean better services, higher standards of care, and safer experiences for patients.

Dr Matthew Cooper, NIHR Newcastle PSRC Safer Integrated Health and Social Care Environments, Research Associate
Dr Matthew Cooper, NIHR Newcastle PSRC Safer Integrated Health and Social Care Environments, Research Associate
Broadening My Understanding of Organisational Culture
Attending the organisational culture working group helped me to broaden my understanding of what organisational culture truly represents. Initially, I viewed workplace culture mainly in terms of supporting staff wellbeing and keeping people happy and healthy at work. Through the discussions, I realised how strongly organisational culture also influences patient safety and the consistent delivery of high-quality care.
Exploring the Ambition of the 10‑Year Plan
The working group explored the ambition of the 10-year plan, which is expected to drive change both during the next 10 years and for the future beyond. This however highlights some key risks:
- That pressure to deliver quickly could lead to rushed decisions,
- Missed input from some disciplines (implementation science for example), or
- Action being taken without full consideration of the plausible impacts (for example removing resources from one service to fund a new idea).
A strong emphasis was placed on transparency of quality of care, including empowering patients through greater voice, choice and access to information. This was balanced alongside clearer accountability and stronger incentives for high-quality care. I was particularly struck by the challenge of double running costs, where services must continue to operate while resources are reallocated, and the importance of deliberately creating time for safety within this context.
Reaffirming the Core Purpose of Organisational Culture
Overall, the working group reinforced that the core goal of organisational culture is to support patients, underpinned by robust checks and balances, compassionate leadership, and a shared commitment to quality and safety at every level of the system. As a team at the NIHR Newcastle PSRC, this is something we are all hoping to reflect on and take forward in our research.
Learn more about the NIHR 10 year plan.