Click below to register
with Francesca Morland

11.30 – 12.30. Howden Room, King George VI building
VCSE Research Partnerships at VONNE
“Working with the Voluntary, Community and Social Enterprise (VCSE) sector in health and care research- VCSE Research Partnerships at VONNE”
Francesca Morland is VCSE Research Partnerships Coordinator at Voluntary Organisations’ Network North East (VONNE). Her role focusses on bringing together the Voluntary, Community and Social Enterprise (VCSE) sector and health and care research sectors, to form more reciprocal and sustainable partnerships.
This session will focus on with the VCSE sector is and how they can be a valuable partner in research. It will include an overview of the VCSE landscape in the region, what they can offer to health research and how to engage effectively with communities through the VCSE sector. Fran will also present what support is available to researchers through VONNE when connecting with communities.
Register by scanning the QR code below or clicking the register here link below.

Pippa Wood NIHR Newcastle PSRC Operations Manager
I went to the NIHR SafetyNet Organisational Culture working group meeting in Birmingham on a cold day in January. I wanted to learn what “organisational culture” means and how it links to patient safety.
So, what is organisational culture?
After listening to researchers from different PSRCs, I learned that organisational culture is basically how people at work get along. It includes the relationships between colleagues, managers, departments, services and different job roles.
How does this affect patient safety?
The way people treat each other at work can directly affect the care patients receive. If communication and relationships between teams are poor, things can go wrong.
For example:
- A patient might be sent home from hospital, but no one tells their family or carers, so no one is there to meet them.
- A family may still be waiting for a call to say they can collect their loved one, only to find out the patient has already been taken home by hospital transport.
But when communication and teamwork are good, patients get much better care.
For example:
- Maternity staff might tell new mothers about breastfeeding support available in their community.
- If an older person is having surgery, hospital staff may work with community care teams and family members to plan what help the patient will need at home.
The biggest thing I learned
If staff are unhappy, feel unappreciated, experience bullied, or feel insecure in their jobs, this can lead to poor communication and bad relationships at work. This can then cause poor-quality services, lower standards of care, and higher risks to patient safety.
But if staff feel happy, valued, and supported, they are more likely to work well together. Good relationships between teams mean better services, higher standards of care, and safer experiences for patients.

Dr Matthew Cooper, NIHR Newcastle PSRC Safer Integrated Health and Social Care Environments, Research Associate
Dr Matthew Cooper, NIHR Newcastle PSRC Safer Integrated Health and Social Care Environments, Research Associate
Broadening My Understanding of Organisational Culture
Attending the organisational culture working group helped me to broaden my understanding of what organisational culture truly represents. Initially, I viewed workplace culture mainly in terms of supporting staff wellbeing and keeping people happy and healthy at work. Through the discussions, I realised how strongly organisational culture also influences patient safety and the consistent delivery of high-quality care.
Exploring the Ambition of the 10‑Year Plan
The working group explored the ambition of the 10-year plan, which is expected to drive change both during the next 10 years and for the future beyond. This however highlights some key risks:
- That pressure to deliver quickly could lead to rushed decisions,
- Missed input from some disciplines (implementation science for example), or
- Action being taken without full consideration of the plausible impacts (for example removing resources from one service to fund a new idea).
A strong emphasis was placed on transparency of quality of care, including empowering patients through greater voice, choice and access to information. This was balanced alongside clearer accountability and stronger incentives for high-quality care. I was particularly struck by the challenge of double running costs, where services must continue to operate while resources are reallocated, and the importance of deliberately creating time for safety within this context.
Reaffirming the Core Purpose of Organisational Culture
Overall, the working group reinforced that the core goal of organisational culture is to support patients, underpinned by robust checks and balances, compassionate leadership, and a shared commitment to quality and safety at every level of the system. As a team at the NIHR Newcastle PSRC, this is something we are all hoping to reflect on and take forward in our research.
Learn more about the NIHR 10 year plan.

By PhD Student Jess McCann
For our October EDI event we welcomed Steve Storey, lead clinical pharmacist at Cumbria, Northumberland, Tyne & Wear (CNTW) NHS Trust, to come and speak to us about how we can make ‘Reasonable Adjustments to create Inclusive Consultations for Patients’.
Reasonable adjustments are described as small, sensible changes made so that people who face barriers to accessing and receiving care, due to a disability, mental health condition or other additional needs, are given equal opportunities.
He explained that we accept reasonable adjustments (like physical ramps, interpreters and assistive technology) in many areas of day-to-day life, so why should healthcare consultations be any different? Within healthcare settings, failing to make such adjustments could worsen existing inequities. For instance, people with un‐met communication, sensory or cognitive needs may experience worse outcomes, including higher mortality, simply because the system assumed a “one size fits all” approach.
In Steve’s session, he spoke of examples of what counts as “reasonable” vs. “unreasonable” adjustments. Sometimes, it isn’t about removing all risk or achieving perfect equality in consultation duration and structure, but about taking practicable, proportionate and effective steps to address disadvantages for that person, at that time. He then moved into an interactive exercise with the audience to experience some of the disadvantages people may face. He asked us to solve a complex mental‐math calculation within 30 seconds; then to try reading some text in a different language; then to try reading very small, blurry text. These simple activities illustrated how patients with cognitive impairment, language barriers, sensory loss or low health literacy are at a disadvantage when seeking, accessing or receiving health care. It was eye-opening to experience the frustration, the delay and confusion that patients are subject to.
Steve discussed several barriers for patients accessing care, such as language and language style, communication that isn’t just about language (e.g., neurodiversity, sensory needs, memory, processing speed), physical disability, diagnostic overshadowing and hypersensitivity (e.g., to sensory stimuli, environments, noise, smells). These may mean that reasonable adjustments to consultations are used; for example, longer appointment times, quieter environments, visual prompts, alternative formats, consultation breaks or bringing a support person to accompany.
Steve shared with us some very impactful real-life examples of people he has provided care for who have required reasonable adjustments, and demonstrated what it means to go the extra mile in delivering person-centred care.

He summarised that reasonable adjustments are not something necessarily taught within university or professional training but are central within professional capability. Being aware of additional needs, asking patients what they would prefer and anticipating barriers and how to act on them allows us to demonstrate humility and advocate for the best possible outcomes for our patients.
It was a very stimulating and thought-provoking session, and it was great to see a big audience of attendees, spanning undergraduate Pharmacy students, postgraduate students, members of the NIHR Newcastle PSRC, wider University network and clinical colleagues from Newcastle upon Tyne Hospital NHS Foundation Trust. The talk provided valuable insights that we can apply not only in our current roles but also take with us throughout our future careers. Engaging with reasonable adjustments in consultation settings may allow us to be better equipped to promote person-centred care to diverse, underrepresented patient groups.
Thank you, Steve!

By Kamil, NIHR Newcastle PSRC Patient, Public Contributor
Lured by the promise of good food and new acquaintances, on Friday 17 October I made my way to Manchester for the NIHR SafetyNet Symposium – a gathering of clinicians, researchers and public contributors united by a single mission: tackling inequities in patient safety. Hosted by the Greater Manchester Patient Safety Research Collaboration (PSRC), the event brought together colleagues from the six PSRCs across England – Central London, Greater Manchester, Midlands, Newcastle, North West London and Yorkshire & Humber.
The day began with coffee and a bustling lobby filled with poster presentations. From the start, it was clear this wasn’t just an academic exercise. It was a collective effort to bridge the gap between policy, practice and lived experience.
One of the first things that struck me was the keynote by Dr Rosie Benneyworth from the Health Services Safety Investigations Body (HSSIB). I hadn’t heard of HSSIB before and I found its mission fascinating. The organisation investigates systemic issues in healthcare topics such as sepsis, prison health and fatigue without focusing on blame. Instead, it looks for learning and improvement. This shift from a ‘who’s to blame’ culture to one of collective accountability resonated deeply with me.
A presentation on avoidable healthcare-associated harm in prisons was another eye-opener. While I wasn’t surprised to hear that prisoners and people experiencing homelessness suffer significantly worse health outcomes, it was sobering to see how these inequities manifest in daily practice e.g. medication shortages, missed appointments and institutional barriers that make basic care difficult. As someone finishing reading a book on health promotion, I could connect the dots between theory and reality: these are not abstract inequalities, they are lived injustices.

One reflection that stayed with me came from a discussion about adoption and breaking cycles of poverty and violence. Even in systems that often feel broken, there are ways to create safety and opportunity through compassion and action.

Several sessions focused on the intersection of communication and safety, including translation and interpreting services. This hit particularly close to home. As a qualified Polish interpreter, I know how vital accurate translation is for patient safety, yet the pay rates offered by NHS providers are often so low that professionals can’t afford to take the work. Hearing that language access was being discussed as a safety issue, not just a convenience, was both encouraging and frustrating. We have the knowledge; now the system needs the will to act.
The Patient Safety Healthcare Inequalities Reduction Framework, presented by Dr Hester Wain, outlined five principles for change: communication and information, training and resources, data, co-production, and research. I was especially struck by her emphasis that the experiences informing the framework are what make it powerful.
By the end of the day, after many conversations in the poster corridor and a moving talk on ethnic inequities in patient safety by Professor Dawn Edge, I left Manchester feeling both hopeful and challenged. The message was clear: health doesn’t happen in a vacuum. Tackling inequity requires empathy, collaboration, and, above all, a commitment to listen to those whose voices are too often ignored. For me, as a patient-cum-public contributor, the symposium was a reminder that my lived experience isn’t just welcome in research – it’s essential.
By Henry Song, Artificial intelligence and data science in multiple long-term conditions theme PhD student
Attending the NIHR Newcastle PSRC/Pharmacy event on the 19th of June was a very positive experience for me. Although I was not able to present my latest research findings due to recent changes in my project dataset, the day still proved to be highly valuable.
I had the chance to see a wide range of presentations from fellow students and colleagues. Some of the work provided direct inspiration for my own research, while others helped to broaden my perspective on the diverse approaches within our field. I was particularly struck by the experimental-based studies on display, which were not only highly innovative but also showed real potential for future impact.
In the afternoon, the workshop on research funding applications was especially useful. It gave me a first insight into the key steps, structure, and approaches involved in applying for research grants. This will no doubt be very important as I continue to develop my academic career.
Overall, the event was an excellent opportunity to learn, connect, and reflect on both my own project and the wider research landscape.
Co-authors: Domna Salonen, NIHR Newcastle PSRC PhD student Haley, Joanne and Carol from the co-development group
Patient safety research considers various matters of life, death and health. These are not any academic topics. For many people, these are experiences they have lived through and are living with.
Before I started my research training, I became a practitioner. Mental health occupational therapy taught me a lot about healthcare and relationships. I learned that it is wise to listen to patients. Two different people can have the same condition, but completely different experiences. I also learned that it is caring to have difficult conversations. At its best, healthcare is about moments when a person in pain gets to talk with someone who is wise and caring. Both the patient and the practitioner use their voice, both listen, both learn.
Now I am learning to research. I have clear boundaries between how I engage with people as a researcher and as a therapist. There are great differences in how to build and navigate relationships in each role. As different as it is to show up as a researcher and as a practitioner, there are some similarities. At its best, also research is about people having good conversations. Researchers and people with personal experience get together to speak, listen and learn.

In my doctoral research, I work with a group of people who I have met through my previous projects. Different group members have personal experiences to share. Some know how it feels to live with addiction, and how it is to recover. Some have been family carers for someone with mental health problems. The common ground is that we all have a strong idea on what mental health support is at its best and at its worst.
We all bring with us our own reasons and motivations to do our bit in research:
Joanne: I want to improve things for others. I want to make positive, long-lasting change easier for everyone: professionals, policymakers, patients, families.
Haley: I want people’s voices to be heard by those who make big decisions at the higher levels. Research is a vital help.
Domna: I research because I want to understand how health systems can grow in wisdom and care. In this group, I can test my ideas and connect with practice memories.
Carol: I want to share my lived experience as a carer by helping with research and use it to help make change for future generations.
Together, we work with clear ground rules. One person speaks at a time, everyone listens. If someone shares a personal story in the room, it stays in the room. We agree and disagree with uncompromising respect. Honesty is essential and expression is free – we can swear, but not at each other.
While we keep the conversation flowing, we get things done. We have spent time talking through the logic behind the project. We have developed information sheets for research participants. We have thought through scenarios that could bring up ethical challenges. We prepare to make sense of data together in the next stages of the research. We have gathered ideas on who to connect with in the later stages of the project, to share findings and learning.
We keep the conversation alive to catch ideas and build new understanding – of healthcare and of each other. We can all agree that hope lives where people sit around a shared table and speak their minds.
A Pre-implementation Study to develop and test an Integrated Discharge Intervention (PreSIDInt study)
As part of a research project funded by the National Institute for Health and Social Care Research, Professor Hamde Nazar and Dr Evgenia Stepanova explore what happens to patients during the transition from hospital to home. In this video, they highlight the essential role of involving patients and the public through meaningful PPIE (Patient and Public Involvement and Engagement).
To ensure a safe and inclusive space for open dialogue, the project established two PPIE groups—a women-only group and a mixed group—each meeting four times throughout the study. These conversations offered crucial insights into real experiences of hospital discharge, revealing gaps in current research and shedding light on challenges that patients regularly face, such as feeling “in limbo”—with limited information, no clear point of contact, and uncertainty about available support.
Hamde and Evgenia reflect on how these contributions shaped the research and deepened its relevance and impact.
Programme Development Grants award NIHR205674 A Pre-implementation Study to develop and test an Integrated Discharge Intervention (PreSIDInt study)


Professor Hamde Nazar sums up the event with PPIE member, Susan Mountain.
On 11th June 2025, the first of a series of events in June focussing on Virtual Wards (hospital at home) was hosted by the Newcastle NIHR PSRC. Representatives across many of the PSRCs contributed to the planning and organisation of this SafetyNet event.
Given the increasing drive for the use of technology in healthcare, the event brought together practitioners, researchers and patient and public representatives to discuss and consider the opportunity and challenges of the use of technology to support virtual ward service delivery.
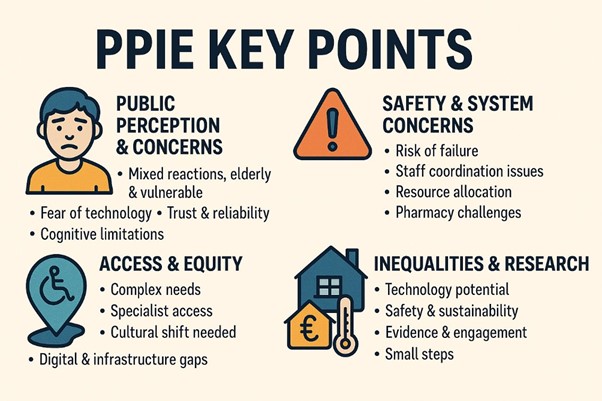
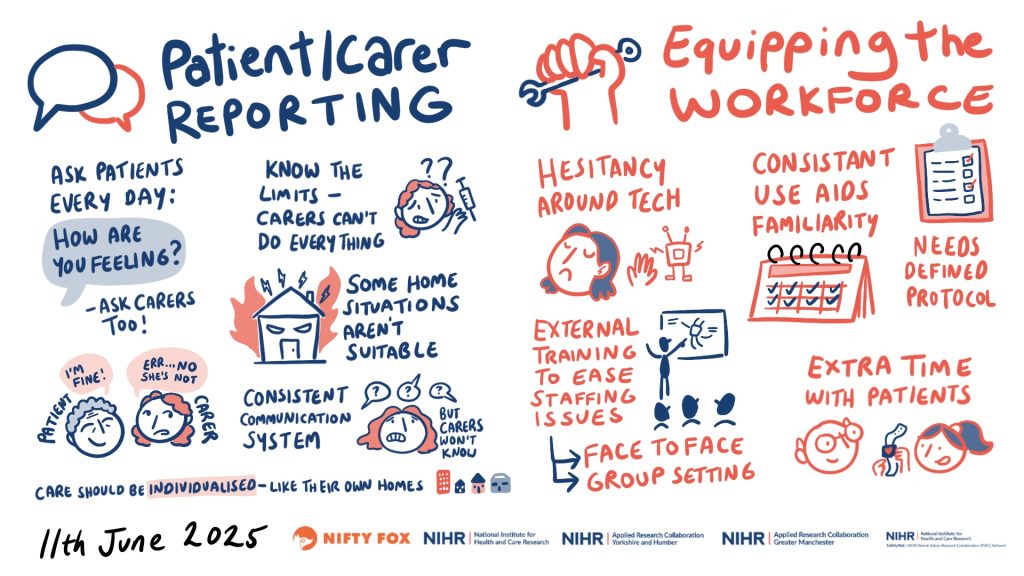
The day started off considering the patient and public voice first and foremost. The figure below summarises discussions from a patient and public involvement and engagement (PPIE) session held earlier in the year. Concerns were aired about the feasibility of technology being appropriate and accessible to all people, with other considerations voiced about the reliability of technology and trusting its effectiveness and security. People acknowledged that there are key challenges to address within the system around the workforce being properly resourced and trained, and about the existing IT infrastructure being fit for purpose. By the end of the discussion, people had ‘warmed’ to the idea, appreciating the opportunities for efficiency and potential improvements in care. However, people were keen to see small incremental developments with rigorous monitoring and evaluation to ensure people and patients were able to keep up and be reassured about the safety, equity and effectiveness of technological advancements within the NHS.
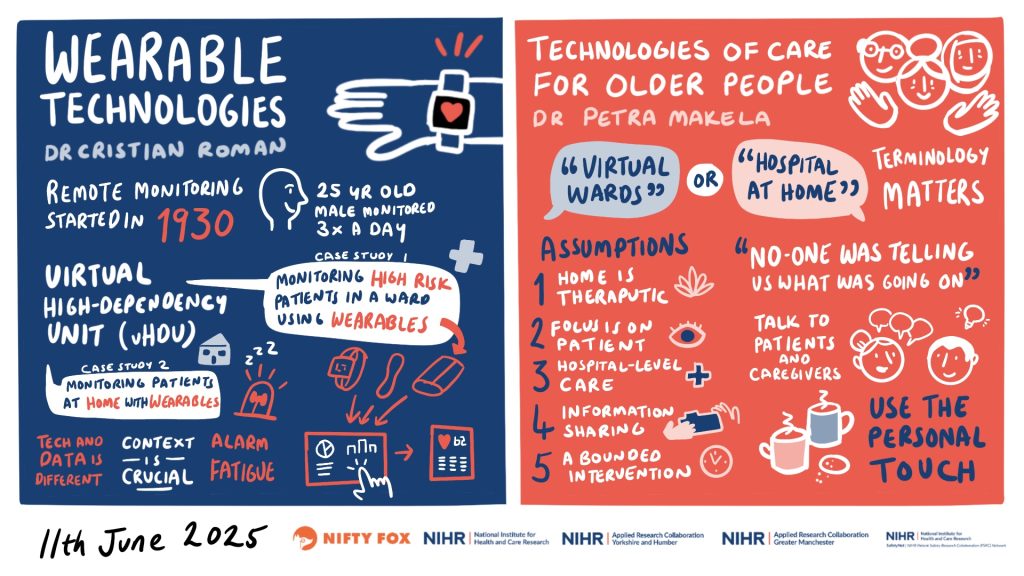
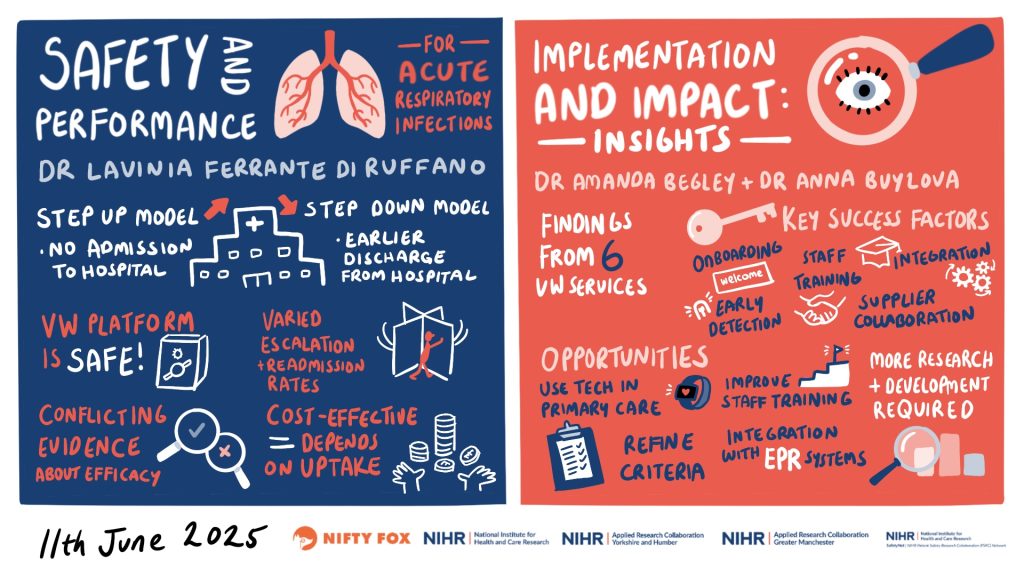
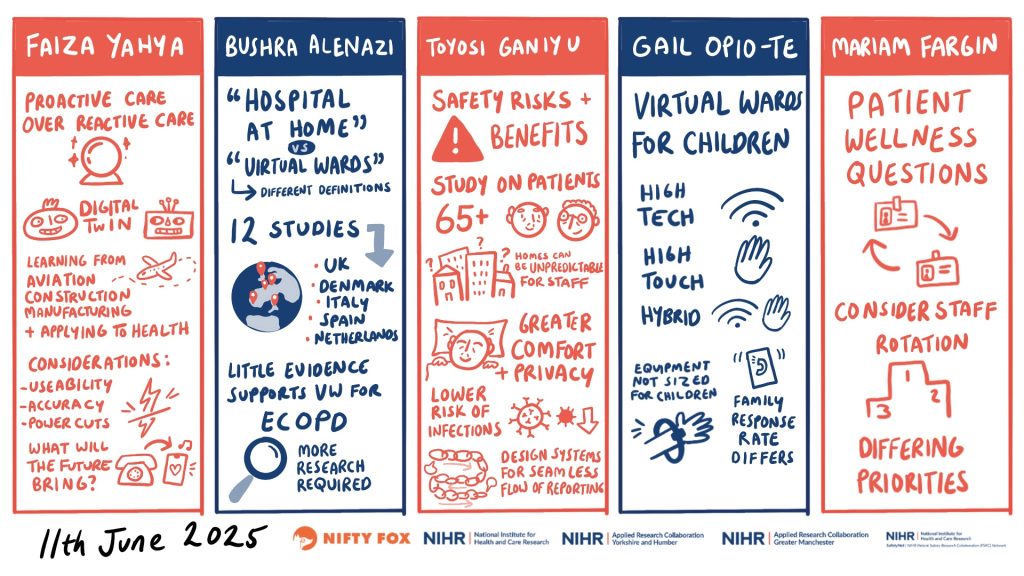
The event then included keynote speakers providing insight into existing evidence for the use of technology, with regards to effectiveness, impact on clinical outcomes and economic repercussions. These have been well captured in a series of scribes created by Claire Hubbard from Nifty Fox Creative.
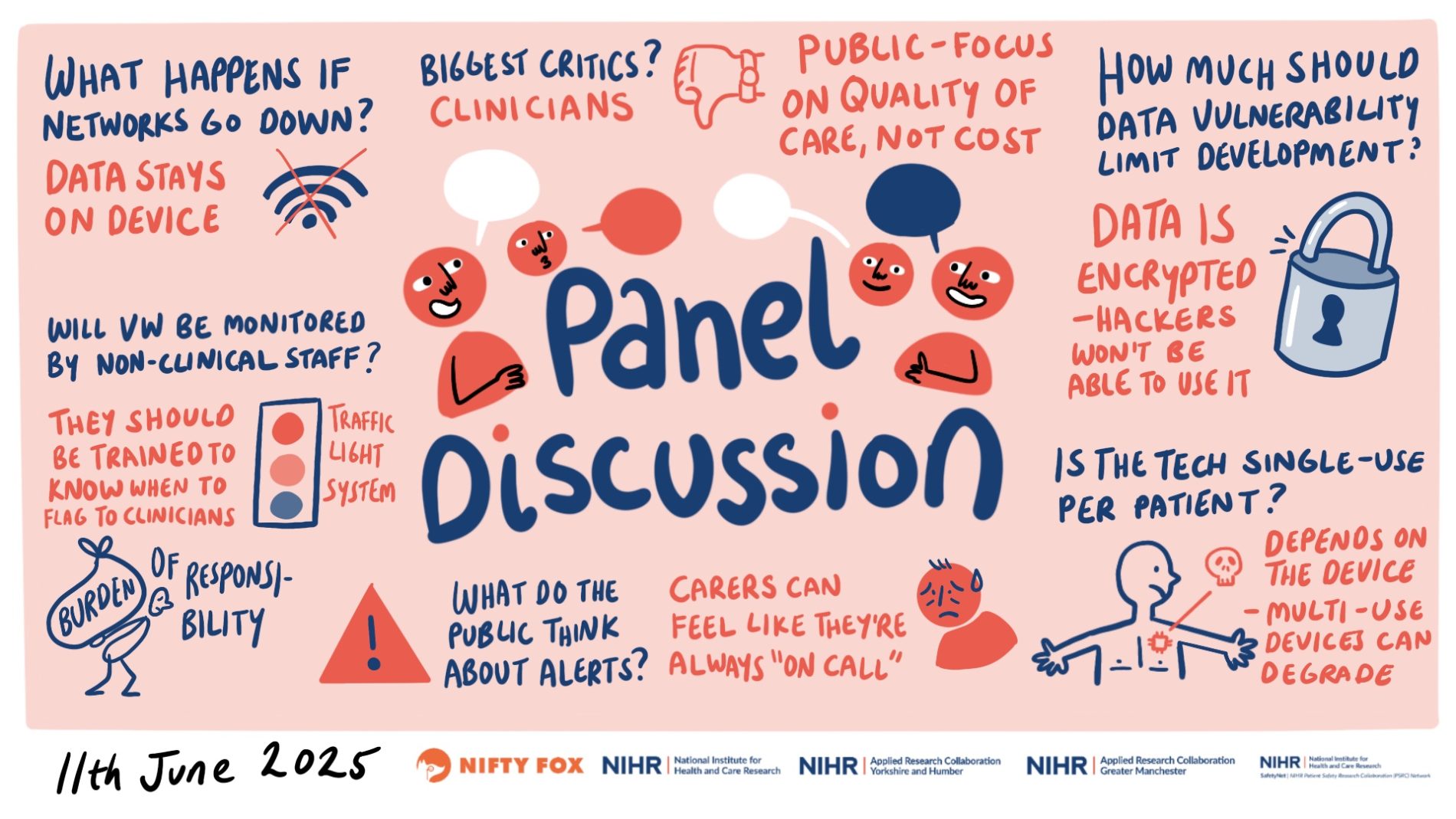
The final panel discussion saw the keynote speakers tackling provoking questions posed by the audience, e.g., ‘how do we ensure equity in technology-enabled virtual wards?’, ‘what are the biggest challenges for the implementation of technology?’, ‘how sustainable is the use of technology in virtual wards?’
There was rich debate, and we can safely say we did not go away with all the answers. Virtual ward care, and technology use in this service model is a quagmire of half-knowns and unknowns. There is need for scrutiny and evaluation of service models to understand what is working, where, how and for which patients and their carers.
The recently released NHS 10-year plan frames technology as the default mechanism to engage with health by 2035. This means trying to understand how technology is deployed and used in virtual ward care is crucial and continued resource and engagement across practitioners, researchers and public and patient representatives is needed.
On that note, one of our patient and public representatives who attended the event provides her experience and takeaway thoughts:
My name is Susan Mountain and I live with multiple long-term conditions. I became involved with public involvement in 2019 and since then I have been part of many research projects, I am a public contributor to the PSRC, AI Multiply, ARC, CNTW, Sunderland University PCPI team, a campaigner for smoking cessation and I help with the Secure Data Environment.
I attended the SafetyNet Technology Enabled Virtual Wards event and found it very interesting. I heard many people talk of virtual wards but to be honest no one really convinced me that they are currently safe. I personally don’t think they are looking at the families that are involved when a patient is sent home using the virtual ward apparatus. I am concerned that there will be too much pressure on the family.
On that note, one of our patient and public representatives who attended the event provides her experience and takeaway thoughts:
I understand that there are benefits: it reduces the pressure on hospital beds; research has shown people recover quicker in home settings and it reduces the chances of infections in recovering patients.
They talked about patients being provided with medical devices to track vital signs and that all data would be transmitted to the hospital where it will be checked at regular intervals. It did worry me if the internet stops working, then how can they monitor. I had an elderly Mam in hospital and even in hospital I had to advocate for her so what would happen if she was at home?
I believe the PSRC has an important role to play in ensuring that this is fully researched before it is rolled out. It is also vital that staff are properly trained and that there is appropriate internet access in the cases selected for treatment at home.
Blog 1
Raising awareness of the unpaid, unselfish work unpaid family carers do.
I wondered if this group was genuinely interested in involving carers in its research. I knew Tilly Hale from Liver North, a brilliant organisation where we had talks with leading consultants and I felt valued and learned a lot.
The Tilly Hale Carer research group inspires me in my own research to raise awareness of the unpaid, unselfish work unpaid family carers do. The involvement of NIHR as funders adds strength for me that the group is genuine. The group helps me to meet others like me, albeit with different reasons for caring. I feel a little less isolated and my voice is heard with this group. In hospitals, carers need a stronger sense of inclusion in decision making and being involved in the triangulation of care as they have knowledge of the patient (and possibly power of attorney).
I was a senior nurse in the NHS in Scotland and left to support a loved one. He was a brilliant academic but also an alcoholic. I have had a roller coaster journey navigating basic care at the point of need and all the horrors of alcoholism in the family. I genuinely thought he would die of injury through intoxication, or refusal of treatment from all services. I feel the patient is often consulted without the family or carer present, so the patient is often not giving informed consent.
Following my work and being part of the Tilly Hale Carer Research Panel, I am preparing a poster for a Glasgow dementia conference in May to raise awareness of the vital work carers do.
Public Contributor: Anonymous

Blog 2
Speaking openly and publicly about my experience brings some relief, knowing that health professionals and researchers want to hear the “good, the bad and the ugly” about failures of health care in the UK, is refreshing.
Hello, my name is Roy Fussey, and I’d like to share my and my wife Elizabeth’s story with you today. During the summer of 2003, Elizabeth, a long-time mental health Nurse went into work and suffered a serious assault from a sectioned patient. This assault has led to Elizabeth developing complex physical and mental health problems.
Since the assault, Elizabeth has been diagnosed with borderline personality disorder and is registered blind. She has put herself at risk, repeatedly leaving the house in an unsafe state, running towards traffic and taking overdoses. Over the years she has attempted to take her life on several occasions, abused alcohol and prescription drugs. In the years since the assault on Elizabeth, I have faced many challenging situations, many caused by her unpredictable and dangerous behaviours that often appear out of her control. Other challenges have been created by services either being unwilling or unable to provide appropriate and timely treatment and care for Elizabeth’s complex needs. On occasions simply discharging her and hoping her problems will go away.

For over twenty years my life has been a challenge and an “emotional roller coaster” at times not knowing what the next day will bring. I believe I am well placed to engage with Health Care public consultation. I have learned what works and what doesn’t. Speaking openly and publicly about my experience brings some relief, knowing that health professionals and researchers want to hear the “good, the bad and the ugly” about failures of health care in the UK, is refreshing. Being able to talk about my experiences brings some relief to me but also can be emotional and troubling.
I have been involved with several research projects with Newcastle University and involved with mental health Trust projects and staff development around carers and family members. I have considerable interest in personality disorders, and I believe it is still an area of health care that is still not fully understood or provided for. The effects on family members living with a person with complex needs can often easily be underestimated by services.
My motivation to participate in research and development is that no other person, family or carer should face the lack of understanding, empathy and failures we have faced on so many occasions. On a positive note, at the moment our lives remain difficult but stable. Brought about by consistency, understanding and empathy from services. But all this we had to fight for!
Researchers should not forget to inform all participants of the outcomes and how the research will be used.
Public Contributor: Roy Fussey