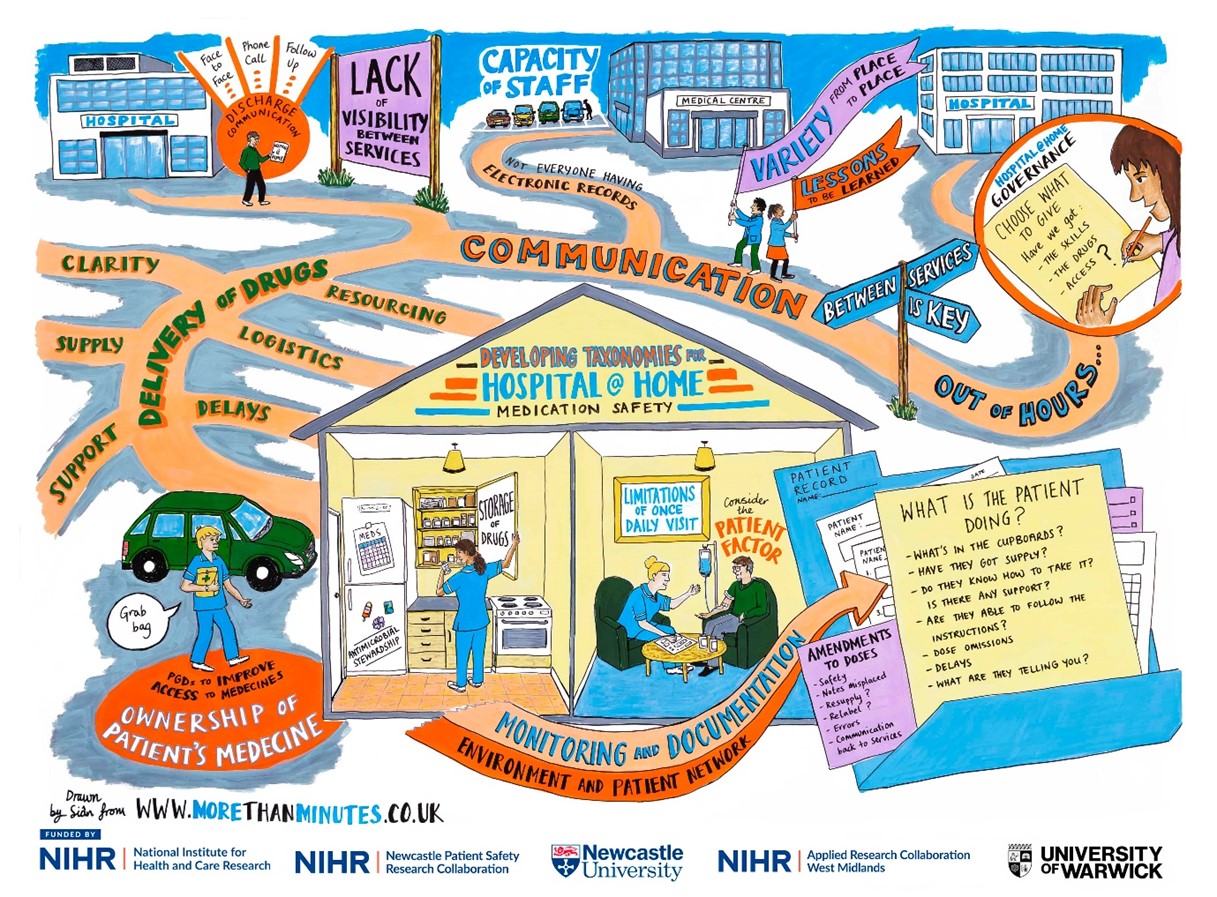
Figure 1 above
How it all began?
I remember attending my first Hospital at Home Society conference in 2024. At this point, I was in the early days of the PhD, eager to learn more about current developments in this research area. During the networking breaks, I remember introducing myself to keynote speakers and little did I know that this would be the start of a wonderful collaboration and supervision for the NIHR SPARC Award.
I was keen to discuss the priority research areas for Hospital at Home (H@H) and later that year, I came across the NIHR SPARC Short Placement Award for Research Collaboration | NIHR. I felt that this was a wonderful opportunity to work with a research team that had the expertise in H@H, who operationally had the research knowledge, the technical and practical expertise in this field, and the existing networks that I could learn from and engage with moving forward. Additionally, my aspirations for professional development to become a clinical academic drove my passion to work with a group of dedicated and trailblazing clinical academics. I felt this would strengthen my experience, especially when considering post-doctoral opportunities.
What is the SPARC award for?
The NIHR SPARC Award allows NIHR academy members to spend time with researchers across other NIHR infrastructure to enhance their personal and professional development and research training experience. From speaking to previous candidates, I learned that this is usually either to develop skills in particular research methods, or to develop collaborations and expertise from researchers in a particular field.
What I did?
The application itself allows you to be quite flexible in how you undertake the placement, which is helpful depending on what you want to achieve. Personally, I had set out 1 day a week over 9 months, whereas other previous applicants undertook it in block placements (e.g. in a 4-week block).
During the placement I managed to conduct clinical visits to H@H services to get the first-hand practical experience. I attended clinical meetings and research meetings linking in with other health tech research centres in the NIHR infrastructure. As part of the award, I also accounted for attending courses and conferences around implementation science and knowledge mobilisation which I felt would be useful for my professional development and demonstrating meaningful impacts with research. The bulk of the collaborative work centred around working on a multi-phase research project. This involved a literature review and arranging an online stakeholder workshop with clinical experts nationally to discuss the findings. This also involved working with a visual minutes artist and presenting the findings at the UK Hospital at Home Society Conference 2026, at the Royal College of Physicians in Edinburgh, which supported input into the survey with H@H practitioners.
Outputs of the placement?
This placement allowed us to develop a Taxonomy of Medicines Safety in Hospital at Home which is aimed for upcoming publication. This enables a better understanding of the concepts of medicines safety in H@H and the links between them. Although the aim of the placement is professional development, I was fortunate to have an abstract accepted for oral presentation at the UK Hospital at Home Society conference in 2026, which is planned for submission to the Journal of Advanced Home Medicine. Additionally, a visual minutes graphic produced from this work is displayed below (See Figure 1).

Blog produced by Faiza Yahya (PhD Candidate), with acknowledgements to the support and supervisory team at the University of Warwick (Professor Daniel Lasserson, Dr Ciara Harris, Sophie McGlen) and the NIHR for funding this award. Appreciation also goes to the Academic Career Development Leads (Newcastle University and NIHR ARC West Midlands) for making this happen.
When “help” might harm: understanding the safety of social prescribing
Social prescribing has become a cornerstone of person-centred care, connecting people to community support, reducing pressure on services, and improving wellbeing. But what happens when these interventions don’t go as planned?
In our recent study, we looked beyond effectiveness to explore an underexamined issue: the potential harms of social prescribing. Using a global umbrella review of existing evidence, we developed a “dark logic” model (a way of mapping how unintended negative consequences might arise).
What did we find?
While social prescribing can offer important benefits, the evidence base highlights several areas of potential risk:
- Mismatch between needs and services – when referrals don’t align with individual circumstances, leading to frustration or disengagement
- Equity concerns – where access to community resources is uneven, potentially widening inequalities
- Burden transfer – shifting responsibility onto individuals or overstretched voluntary sector services
- Psychological impacts – including feelings of stigma, rejection, or failure if support pathways break down
Importantly, many of these harms are not the result of single decisions, but emerge through complex systems of care, commissioning, and delivery.
Why this matters for patient safety
Patient safety conversations have traditionally focused on clinical interventions. Our findings suggest we need to extend that thinking into community-based and non-medical models of care.
Social prescribing operates across organisational boundaries (primary care, local authorities, and the voluntary sector) which can create gaps in oversight, accountability, and follow-up. Without careful design, implementation, and evaluation, there is a risk that well-intentioned interventions could inadvertently contribute to harm.
What can we do differently?
Our “dark logic” model is not about discouraging social prescribing, but about making it safer and more equitable. Key implications include:
- Building safety considerations into service design from the outset
- Strengthening monitoring of outcomes beyond uptake and satisfaction
- Supporting the voluntary and community sector to deliver sustainable services
- Ensuring equity is a central focus in referral pathways and access
- Recognising and addressing the emotional and psychological experiences of participants
Looking ahead
As social prescribing continues to grow, there is an important opportunity to embed patient safety principles into its development. This means moving beyond asking “does it work?” to also asking “for whom, in what contexts, and at what cost?”
By bringing a safety lens to this evolving area of practice, we can better ensure that social prescribing delivers on its promise, without leaving unintended harms unseen.
Call to action
We encourage researchers, practitioners, commissioners, and community partners to actively incorporate safety thinking into social prescribing policy and practice. This includes:
- Designing services with potential harms in mind, not just intended benefits
- Sharing learning on unintended consequences across organisations and sectors
- Embedding routine monitoring of safety outcomes in evaluation frameworks
- Involving patients and communities in identifying what “safe” support looks like in practice
By working collaboratively and proactively, we can ensure that social prescribing not only supports wellbeing, but does so safely, equitably, and sustainably.
Paper link – https://bmjopen.bmj.com/content/16/5/e108998.abstract
Dr Matthew Cooper
Yahya F, Cooper M, Saif W, Kassem M, Nazar H Development of a Hospital at Home Digital Twin for Patients With Frailty: Scoping Review Journal of Medical Internet Research 2025;0:e0 URL: https://www.jmir.org/2025/1/e81510 doi: 10.2196/81510
What’s this about?
How can we make the most of advanced technology and live information to improve how we deliver hospital-level care at home?

What’s this about?
How can we make the most of advanced technology and live information to improve how we deliver hospital-level care at home?
Why are we looking at this?
The NHS 10-year plan wants to:
- Move more care from hospitals closer to home
- Prevent illness instead of just treating it
- Use more digital tools to support care

What is the work we are doing?
We explore all three by using something called Digital Twins. A Digital Twin is like a live virtual simulation of a patient and their surroundings using real-time information. It can help healthcare professionals predict problems early, to give care that’s safer and more personalised.
Learning from, and working with other experts, our work looked at creating a simple step-by-step model, which can be used to develop a Hospital-at-Home Digital Twin. This review was based on existing evidence for tools to support this, for patients living at home with frailty.
What does this mean?
- Technology and real-time data can help health professionals care for patients at home more efficiently.
- Digital Twins could make care timelier, safer, and tailored to each person.
- We’ve outlined the main building blocks for creating a Hospital at Home Digital Twin.
This work is just the beginning, but it shows how technology could possibly change the world of healthcare and what needs to be worked on to make this possible.
For those that want to know more:
Our article reviews the current evidence for tools that exist to support the development of a Hospital at Home Digital Twin. We describe the 5 layers required to build a Digital Twin. Results show that a variety of technologies exist to pick up information, such as wearables. However more understanding is needed of how we manage that data, store it, translate it and use it to make useful predictions to help staff who are looking after us make decisions. This article also talks about some of the challenges and opportunities we may face when using these technologies in our current healthcare system.
By Safer Integrated Health and Social Care Environments PhD Student, Lauren Lawson
In August I was lucky enough to have the opportunity to travel to Singapore to attend the BMJ International Forum on Quality and Safety in Healthcare. I presented a poster about a service evaluation I had worked on, led by Dr Matt Cooper, which explored a hospital discharge service providing one-to-one, personalised support for carers of people leaving hospital.
The conference theme, moving together toward sustainable quality, emphasised the importance of collaboration across sectors to achieve lasting improvements in healthcare. Many sessions focused on involving patients and carers as partners in care, by embedding lived experience into service design and evaluation to make change meaningful and sustainable. Other sessions explored how to support population health across the life course, recognising the social factors that shape health and the role of community-based care.

“For me, a key message was that sustainability in healthcare also depends on continuity, where good care extends beyond the hospital to meet people’s needs in the community.”
These messages echoed the key findings from our service evaluation, which highlighted how person-centred, inclusive support can empower carers to support their own wellbeing and the patient during hospital-to-home transitions. Our approach of working with staff and carers to understand the service’s impact reflected the same emphasis on participation and learning that was central to the conference. For me, a key message was that sustainability in healthcare also depends on continuity, where good care extends beyond the hospital to meet people’s needs in the community.
After the conference I got to explore Singapore and think about sustainability in a different way. The contrast between greenery and skyscrapers, the hawker centres blending food from diverse communities together, and the evening light show through the Supertrees were all incredible reminders the benefits of collaborative design.

By Safer Integrated Health and Social Care Environments theme Research Assistant, Evgenia Stepanova.
The PreSIDInt study research team recently presented at The Future Is Cultural: Policy, Practice, and Education Congress, held at the Universitat Internacional de Catalunya in Barcelona (15–17 September 2025). Read more about the event here. The conference was well attended, bringing together an international mix of academics, policymakers, practitioners, artists, and community representatives.
Our paper, “Culturally Competent Strategy to Research: Recommendations and Measures to Design, Deliver and Disseminate a Research Study,” was presented in the Audience Analysis and Cultural Participation session, alongside several thought-provoking contributions. These included presentations on festival resilience (Piotr Firych, Adam Mickiewicz University, Poland), festivalization and its links to social change and democracy (Emmanuel Negrier, University of Montpellier, France), students’ cultural practices and emotions (Marine Thebault, Université Côte d’Azur, France), and participatory evaluation within the Stronger Peripheries Project (Elisabete Tomaz, ISCTE, Portugal).
Whilst other presenters examined how culture is embedded in communities and its role in shaping social change, democracy, and territorial identity, our work focused on how culture and cultural identity can be explored within the research process itself. This generated strong interest, with attendees taking photos of the findings and engaging in lively discussion around our interactive online tool. Leaflets featuring artwork illustrating the project’s key findings were also distributed and well received, with many participants taking them on board. These exchanges provided valuable feedback, informed next steps, and strengthened the project’s international visibility as we continue developing the framework into an accessible online resource.

A Pre-implementation Study to develop and test an Integrated Discharge Intervention (PreSIDInt study)
As part of a research project funded by the National Institute for Health and Social Care Research, Professor Hamde Nazar and Dr Evgenia Stepanova explore what happens to patients during the transition from hospital to home. In this video, they highlight the essential role of involving patients and the public through meaningful PPIE (Patient and Public Involvement and Engagement).
To ensure a safe and inclusive space for open dialogue, the project established two PPIE groups—a women-only group and a mixed group—each meeting four times throughout the study. These conversations offered crucial insights into real experiences of hospital discharge, revealing gaps in current research and shedding light on challenges that patients regularly face, such as feeling “in limbo”—with limited information, no clear point of contact, and uncertainty about available support.
Hamde and Evgenia reflect on how these contributions shaped the research and deepened its relevance and impact.
Programme Development Grants award NIHR205674 A Pre-implementation Study to develop and test an Integrated Discharge Intervention (PreSIDInt study)


During the summer of 2025, Dr Matt Cooper and Dr Charlotte Richardson hosted four undergraduate and postgraduate students at Newcastle University to complete a research internship. Three of the interns have reflected on this experience.

Imogen Tate (BSc Hons Psychology with Professional Placement)
I am currently a BSc Psychology with Professional Placement student going into my 4th year (stage 3), and this summer I completed a month internship working on the scoping review ‘Caring for the Carer: What are the active ingredients of interventions supporting informal carers’ wellbeing and welfare needs?’ under the supervision of Dr Matt Cooper.
I was supported to title and abstract screen using Rayyan, full-text screen and data extract, and conduct a promise analysis of the included papers. This experience has significantly developed my research skills for scoping/systematic review. Notably, I have enhanced my problem-solving skills for refining a research question throughout this process, as a high volume of papers were initially included; I enjoyed the collaborative nature of evaluating the project’s direction when problems arose. I am looking forward to seeing the meaningful impact on carer wellbeing that the project will have.
I am so pleased to have had the opportunity to attend the 2nd annual NIHR Newcastle PSRC and School of Pharmacy Conference 2025 in my first week, as it gave me great understanding of the scope of the work that is conducted within the department and provided insight into where my psychology background is advantageous.
I particularly valued working in such a welcoming and supportive environment surrounded by fellow interns and PhD students with such a wide range of research interests. This experience has reaffirmed that I would love to pursue a PhD one day and eventually a career that has a platform for both clinical and academic practice!
Neave Woollam (BSc Hons Psychology with Professional Placement)
I am currently an undergraduate psychology with professional placement year student at Newcastle University, and this summer I completed a four-week long internship supervised by Dr Matthew Cooper. The project was a scoping review looking at interventions to support carers’ wellbeing and welfare needs.
This created a great opportunity for me to develop my research and professional skills. Including learning to use a new software (Rayaan) to screen papers, doing data extraction and a promise analysis. When our original search returned an overwhelming number of papers, it was really interesting to see how the search was refined to deal with this. This gave me insight into how to tailor search strategies when conducting a scoping review.
I enjoyed working in an office alongside other interns and PhD students. I loved hearing about the different topics being researched and the range of methodologies being used to do so. It really opened my eyes up to the possibilities within pharmacy research and made me realise it’s not all lab based. I especially enjoyed hearing about the Patient and Public Involvement (PPI) work that informed this review. Seeing the coproduced artwork really inspired me and made me think about PPI in research more creatively.
Overall, I hope to continue using the skills, knowledge and experience I have gained over this internship in my final year of university and in my career.
Tom Collis (MSc in Data Science and Artificial Intelligence)
Hi, my name is Tom, I am currently studying an MSc in Data Science and Artificial Intelligence at Newcastle University. Prior to this I studied Medicine at Newcastle University, and I subsequently completed my Foundation Years, and a Clinical Teaching Fellow Year. In June and July 2025 I undertook this fascinating research internship with the School of Pharmacy, under the supervision of Dr Richardson and Dr Cooper.
The internship project involved a systematic review exploring the roles and experience of caregivers in virtual wards. With the NHS aiming to move more care from inpatient hospitals into the community, virtual wards, with the support of caregivers, will be fundamental to facilitating this shift in the location of patient care. The role and experiences of caregivers within virtual wards is an under-researched area, and this systematic review aimed to provide an overview of the existing literature, and a guide for future research projects.
This internship was greatly rewarding, educational, and enjoyable. Working within a team of driven academics was inspiring and has further fuelled my passion for working within academia. Being based in the Newcastle Patient Safety Research Collaboration office gave me an insight into the valuable work being undertaken at Newcastle University, aimed towards improving patient safety and care. The skills and knowledge I have gained from the internship, in particular how to conduct a systematic review, have been invaluable, and have given me a strong foundation to build upon in my future training. Additionally, being involved in the design of the systematic review, and all stages of its undertaking, meant I developed an insight into the complex nature of carrying out research, and how obstacles can be overcome through teamwork, communication, and lateral thinking. I have no doubt that this experience has developed my research skills and will underlie all future work in academia that I hope to undertake. Thank you very much Dr Richardson and Dr Cooper for this opportunity, and your support!
By Dr Matt Cooper, NIHR Newcastle PSRC, Safer Integrated Health and Social Care Environments Theme Research Associate.
Over the past year of the Tilly Hale Carer Research Panel, we have met on several occasions both in person and online. The sessions have been hugely beneficial to both myself and our research team. The purpose of the group was to establish a collaborative space where carers could help priorities and set the agenda for the research we are doing within the school and patient safety group. Initially I found it difficult to work out how to ensure the group made an impact and how we could become sustainable beyond the funding. I worried that the group would not have a single direction, and I wanted to ensure I brought meaning and a purpose to the group. Looking back over the past year I think the group has made more impact that I initially would have realised.
Since the group was established, I have had the absolute honour in being able to listen and learn from the experts in what caring should be about, the challenges they face, and where we need to be doing more to research to support the development of services. The carers in the group are passionate about providing the best support for the people they care for, while providing a selfless act of giving their time and energy, despite the challenges they face or the impact on their own health and wellbeing.
The group has informed my thinking and critical review of research more that I had accredited before, and they have made me think more holsitically about the research we can do. Within our research team we now have 7 projects in this space including, student carers, carers involvement in medication management, carers involvement in hospital at home care, carer wellbeing, and support for ethnically marginalised carers. All these projects I believe have been informed by the panel and give thanks to them and their openness to support this.
Of course, we are also working on an art piece which has been commissioned around what it means to be a carer, and below is an intial draft of this. This piece I hope can be sent far and wide to demonstrate the vitally important role carers play in the healthcare landscape and support the research we are doing. I thank the research panel for their honest reflection when developing this piece and I hope that it does justice to their experiences.

Our first NIHR Nrewcastle PSRC Theme Implementation Management Group meeting, thankfully shortened to TIMG, for our theme on safer, integrated care environments was great! It was a meeting that could not have better met its terms of reference. Providing input and advice on the theme direction, priorities, and strategies to investigate them.
We had stakeholders from organisations and sectors who could understand the big-picture problem being addressed in the theme and were generous with their suggestions and signposting. It helped that they were all clearly champions in their fields of work and motivated towards improving practice around integrated care and patient safety.
As a theme lead, getting a steer on the key issues in relation to the topic areas we currently have active projects was invaluable. But the most significant discussion point was about something myself and researchers in our theme had not come across; ‘Shared care’. As soon as this was mentioned as an area of possible interest from our ICB representative, other TIMG members contributed their emotive perspective. This highlighted something that was clearly causing contention in practice on multiple fronts with implications on patient safety, with seemingly little being done to resolve and/or investigate and optimise.
This piqued our interest; something under the radar and causing this much drama was worth investigating. Our first delve into literature was unsuccessful in retrieving anything. Dr Google was more fruitful with a few guidance and policy documents to describe shared care as ‘an agreement to ensure seamless prescribing and monitoring of medicines which enables patients to receive care in an integrated manner’.
This seemed like something we could be looking into. The available documents, however, made this initiative sound quite benign and actually like something that could work out really well for patients. So, why the drama?
The following weekend, I happened to be having a social encounter with a family member, who is also a practising GP. So, over coffee and cake I asked about shared care. I was not prepared for the head-in-the-hands response. The implementation and reality of this agreement in clinical practice sounds messy, complex and potentially riddled with risks to patient care through monitoring, identifying and addressing fluctuations in chronic conditions in patients who are often experiencing multiple long-term conditions and have complex health and social care needs. Also, shared care appears to be here to stay in the NHS…at least for a while.
So, what has this meant for us within our theme; we have started to look at this problem more systematically. Given the lack of published evidence on this initiative, stakeholder engagement will be crucial to understand it better in terms of its design, delivery and implementation, work out the risks and potential benefits and investigate how patient safety is protected and consolidated. It looks like our first TMIG has flagged a potential theme priority…watch this space!
